

Background: Patients with R/R AML, or intermediate-, high-, and very high-risk MDS have a poor prognosis with, respectively, a 5-year survival of <10%, or median overall survival of 0.8 to 3.0 years (https://seer.cancer.gov/, Greenberg 2012). Novel chimeric antigen receptor (CAR) T cell products have had limited clinical success in patients with myeloid disorders due to absence of clear AML-specific target antigens and a hostile microenvironment for T cell-based therapy (Gill 2019, Epperly 2020). Non-engineered allogeneic haplomatched NK cells have shown activity in AML, and are therefore an attractive cell source to develop novel targeted cellular therapies to treat AML/MDS. Complete remission with or without hematologic recovery from 20% to 50% has been noted in patients with R/R AML with non-engineered, allogeneic haplomatched NK cells administered after lymphodepletion with minimal cytokine release syndrome or neurotoxicity (Miller 2005, Bachanova 2014, Rubnitz 2015, Romee 2016). The cytolytic activity of NK cells arises from a balance of activating and inhibitory receptors; key among the activating receptors is NKG2D. NKX101 is composed of CAR NK cells engineered to express a chimeric NKG2D receptor fused to co-stimulatory (OX40) and signaling (CD3ζ) domains to enhance their intrinsic anti-AML activity. NKX101 also expresses a membrane-bound interleukin-15 to serve as an autocrine growth factor and thereby increase persistence. Preclinical characterization showed that NKX101 has 4- to 8-fold greater cytotoxicity, superior intrinsic longevity, and enhanced anti-tumor activity in AML xenograft models relative to non-engineered NK cells. Hence clinical evaluation of NKX101 is being undertaken in this Phase 1 study in subjects with R/R AML or higher-risk MDS.
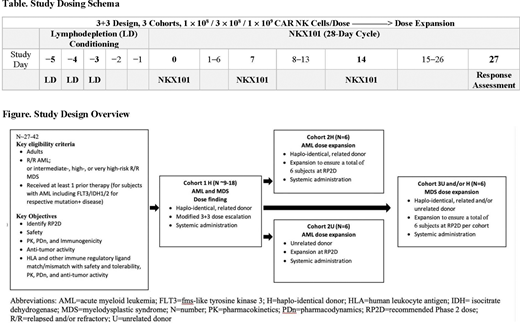
Methods: This is a multicenter, open-label, Phase 1 study of NKX101 (Figure). The study will be conducted in 2 parts: Part 1 (dose finding) to determine the recommended Phase 2 dose (RP2D) of NKX101 utilizing a modified "3+3" enrollment schema. The study will enroll subjects with either R/R primary or secondary AML or R/R higher-risk MDS. Building on existing clinical data referenced above with non-engineered haplomatched NK cells, NKX101 manufactured from NK cells obtained from haplo-identical-related donors (H) will be used in Part 1. Part 2 (dose expansion) will further evaluate safety and tolerability, pharmacokinetics (PK), immunogenicity, pharmacodynamics (PDn), and anti-tumor activity of NKX101 from unrelated, HLA-mismatched donors with separate expansion cohorts for patients with AML or MDS. Each dose is defined by the total number of viable CAR NK cells. The starting dose of NKX101 is 1 × 108 viable CAR NK cells where NKX101 will be administered on Days 0, 7, and 14 of a 28-day cycle following standard fludarabine/cyclophosphamide lymphodepletion. Three dose levels are planned (Table). The primary endpoint is incidence of adverse events, dose-limiting toxicities, clinically significant laboratory abnormalities, and determination of the RP2D. Secondary endpoints include evaluation of standard cellular PK parameters, PDn, immunogenicity, and anti-tumor responses. AML patients will be assessed for efficacy using updated ELN criteria (Döhner 2017) including measurable residual disease assessment, and MDS using modified IWG criteria (Cheson 2006). Exploratory endpoints are correlation of various degrees of HLA and KIR ligand match/mismatch between donor and recipient with primary and secondary safety, PK, and efficacy measures. Enrollment across multiple US sites is expected to start in late 2020.
Bachier:CRISPR: Honoraria; Juno Therapeutics, a Bristol-Myers Squibb Company: Honoraria; AlloVir: Honoraria; Sanofi: Speakers Bureau. Borthakur:Novartis: Research Funding; FTC Therapeutics: Consultancy; Curio Science LLC: Consultancy; BioTherix: Consultancy; Nkarta Therapeutics: Consultancy; Treadwell Therapeutics: Consultancy; Incyte: Research Funding; AstraZeneca: Research Funding; Cyclacel: Research Funding; Argenx: Consultancy; Abbvie: Research Funding; Jannsen: Research Funding; PTC Therapeutics: Research Funding; GSK: Research Funding; Oncoceutics: Research Funding; Xbiotech USA: Research Funding; BioLine Rx: Research Funding; Polaris: Research Funding; BioLine Rx: Consultancy; PTC Therapeutics: Consultancy; BMS: Research Funding. Hosing:NKARTA Inc.: Consultancy. Blum:Syndax: Membership on an entity's Board of Directors or advisory committees; Celyad: Research Funding; Leukemia and Lymphoma Society: Research Funding; Xencor: Research Funding; Amerisource Bergen: Honoraria. Rotta:Merck: Speakers Bureau; Jazz Pharma: Speakers Bureau. Ojeras:Nkarta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Barnett:Nkarta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Rajangam:Nkarta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Majhail:Mallinckrodt: Honoraria; Anthem, Inc.: Consultancy; Incyte: Honoraria; Nkarta Therapeutics: Honoraria. Nikiforow:Kite/Gilead: Honoraria; Nkarta Therapeutics: Honoraria; Novartis: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal